New instruments for canal retreatment, RetreatAll® files
Gaceta Dental echoes this new clinical case where Zarc’s RetreatAll® files and the new endodontic techniques are key when the aim is to save the tooth and thus avoiding apical surgery when endodontics has not fulfilled its objective.
When it comes to avoiding extraction, endodontics is the key. Despite this, later problems may appear for various reasons and the knowledge of the possibilities that the specialist has is extremely important when saving the tooth.
Retreatment combined with current CBCT, magnification and diagnostic techniques is a viable option to avoid apical surgery and keep the teeth. The success rate is around 77%.
For endodontics to achieve its goal, the filling material contaminated by persistent and failure-causing bacteria, must be removed. To do this, the most effective way is to remove the old gutta-percha using rotary instruments to be able to proceed with disinfection and then give way to the three-dimensional sealing of the canal system, which will ensure that the endodontics is successful in the long term.
Clinical case: case of retreatment through the crown of a 36 of a patient previously treated 6 years ago
The patient reports acute pain on percussion with inflammation of the area and functional impotence. After clinical examination, positive percussion and palpation and physiological probing were seen, thus it is established a definitive diagnosis of a tooth previously treated with symptomatic apical periodontitis.
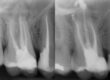
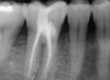
Prior to treatment, radiological exploration with periapical radiography and CBCT is performed to have a three-dimensional view of the case. (Fig. 1) The images show that the roots have radiolucent images, which is why the existence of missed canals is suspected. The existence of root fissures is ruled out. (Fig. 2)

Figure 1. Radiographic study prior to the start of treatment, where we can observe in 2D and 3D the existence of periapical pathology.

Figure 2. Axial plane of the middle third where the existence of cortex around the roots can be observed, ruling out the presence of vertical cracks or fractures.
It is decided to keep the metal-ceramic crown of the molar, so the entire procedure is carried out through it.
Once anesthetized and isolated, the direction indicated by the CBCT is followed until reaching the chamber and locating the old gutta-percha. For its removal, the RetreatAll® system is used, starting with the file Zr1 (04/30, 21 mm) and Zr2 (25/04 25 mm) at 500 rpm, managing to safely remove the contaminated gutta-percha from the previously treated canals. ( Fig. 3)

Figure 3. Images of the Zr1 and Zr2 files of the RetreatAll® system used during retreatment to remove the contaminated gutta-percha within the canal system.
For the omitted canals, the E-conncect S apex locator and the BlueShaper® dual alloy instrumentation system, it is used the sequence from Z1 to Z4.
Once this process is finished in the five canals of the molar, irrigation is carried out. The 4% sodium hypochlorite used for disinfection and the 17% EDTA are activated with the UltraX system in cycles of 30 seconds the first one and a cycle of one minute the second one.
To achieve a good three-dimensional seal, the continuous heat technique is used with the Fast Pack system. The fluid gutta-percha injection Fast Fill system is used to fill the coronal third. (Fig 4 and 5)
The results of the obturation and its subsequent review at 12 months can be seen in the microscope images. (Fig 6 and 7)

Figure 4. Conometry where we can see the arrangement of the gutta-percha inside the duct system.

Figure 5. Sealing unit used for vertical condensation and filling of the middle and coronal third of the
duct system.

Figure 6. Images under the light microscope and radiographs, where we can observe the three-dimensional sealing of the root network.

Figure 7. Revision X-ray 12 months later
Discussion
The success of complex cases depends fundamentally on a good diagnosis of the cause of failure since, if it is a fissure, for example, there is no endodontic solution.
In this specific case, CBCT provides us with a three-dimensional view that is key to determining the cause of this failure, which is the existence of two omitted conduits and lack of condensation in the old fill.
3D allows us to see images that often go unnoticed in periapical radiographs.
To remove the old filling, the fastest and most effective option is the mechanized instrumentation. The activation of the irrigating fluid is crucial to minimize the bacterial load. To conclude, the three-dimensional filling is crucial to ensure success and that a colonization of microorganisms does not occur again, which is what produces a new failure. The more the bacterial load is reduced and a good three-dimensional seal is made, the apical periodontitis will disappear and will not recur.
Conclusions
If you want to know the conclusions and the debate generated by this clinical case, read the full article published by Gaceta Dental here.

Dr. Rafael Cisneros
Professor of Endodontics at the European University of Madrid. Director of the Master’s Degree in Advanced Endodontics at the same university. Doctor of Dentistry. Former president of the Spanish Association of Endodontics (AEDE). National and international speaker. Author and co-author of several articles published in endodontic impact journals. Exclusive endodontist in Madrid.

Dr. José Aranguren
Exclusive endodontist, he completed his degree in Dentistry at the European University of Madrid and is currently director of the Master of Advanced Endodontics at the Rey Juan Carlos University (Madrid) and professor at the International Dental Institute in Palm Bleach (Florida). Speaker of courses and conferences at national and international level. President Elect of AEDE. Member of the COEM.

Dr. Roberto Estévez
Dr. Roberto Estévez is a doctor of dentistry and works as a professor of Dentistry, a professor of Tutored Practices I / II and a professor contracted with a doctor by ANECA. He is also coordinator of the Master’s Degree in Advanced Endodontics and editor of the Official Journal of the Spanish Association of Endodontics. Exclusive practice in (Endodontic Clinic Madrid)

Dr. Francisco de la Torre
Currently dedicated exclusively to endodontics, he completed his degree in Dentistry and specialized in Endodontics at Universidad Europea in Madrid. He then completed a Doctor of Dentistry degree, with a thesis on the connection between periapical lesions and diabetes. He is the author and co-author of numerous articles in reputable endodontic journals. Best clinical case award at the AEDE 2009 congress.
More information
If you are interested in any of our products, please contact us. We have a team of endodontic specialists who will be happy to help you.
Write us an email at hola@zarc4endo.com.